Tremendous suffering is all around us, and the crisis is not improving. People are desperate for jobs, security, and the most basic necessities of life. The conflict between good and evil is more palpable than ever. Most every day, we hear gunfire, usually far enough away to avoid being startled, sometimes not.
At the same time, we can hear hymns from churches around us, and kids give us fist bumps with smiles on their faces after life-changing operations.
Our hearts ache as we pray for the American nurse and her child kidnapped near Port au Prince last week. We do not know her or what part of town she was in, but the story is quite terrifying. It almost seemed things were getting a little better for a while, but now the situation has intensified. What you don’t hear in the news is that many good people here are just trying to live life, love each other and provide for their families.
Why are we still here? It is no small miracle that our hospital is fully functional and taking care of more people than ever before in its 42-year history. Everything is more difficult these days. Sourcing materials and supplies is challenging, expensive, and sometimes life-threatening for our staff. But we still do it because people come with life- and limb-threatening injuries and illnesses to Hôpital Adventiste every day. They depend on us. Life is tough at baseline, but when tragedy and sickness occur, there are few options.
Clifford’s Life-Changing Surgery
Clifford did not have a life- or limb-threatening injury but was born with osteogenesis imperfecta. This genetic defect in collagen production often results in fractures and deformity. Believe it or not, he could still walk with his curved legs! His shins were skinned up from hitting the ground when he walked uphill.

Conor Spady, who just finished his one-year fellowship in Global Orthopedics at HAH, stands with Clifford before surgery.

Amazingly, Clifford’s ankles are flexible enough to accommodate this deformity.
The surgery is not complicated, but being able to do a first-rate job depends on many details. Surgical implants, a functioning autoclave, trained staff, C-arm for taking x-rays in surgery, an anesthesia machine, monitors, bandages, oxygen, and electricity are all essential and require significant effort to maintain in this environment. Living in what is justifiably a war zone can sometimes force us to prioritize the urgent over the important. And we do a lot of the urgent. Clifford’s surgery was not urgent, but it was life-changing for him and his family. It is particularly special that even without a life or death problem, he can still come to Hôpital Adventiste, in a war-torn country with minimal resources and experience the kingdom of God and the miracle of healing.

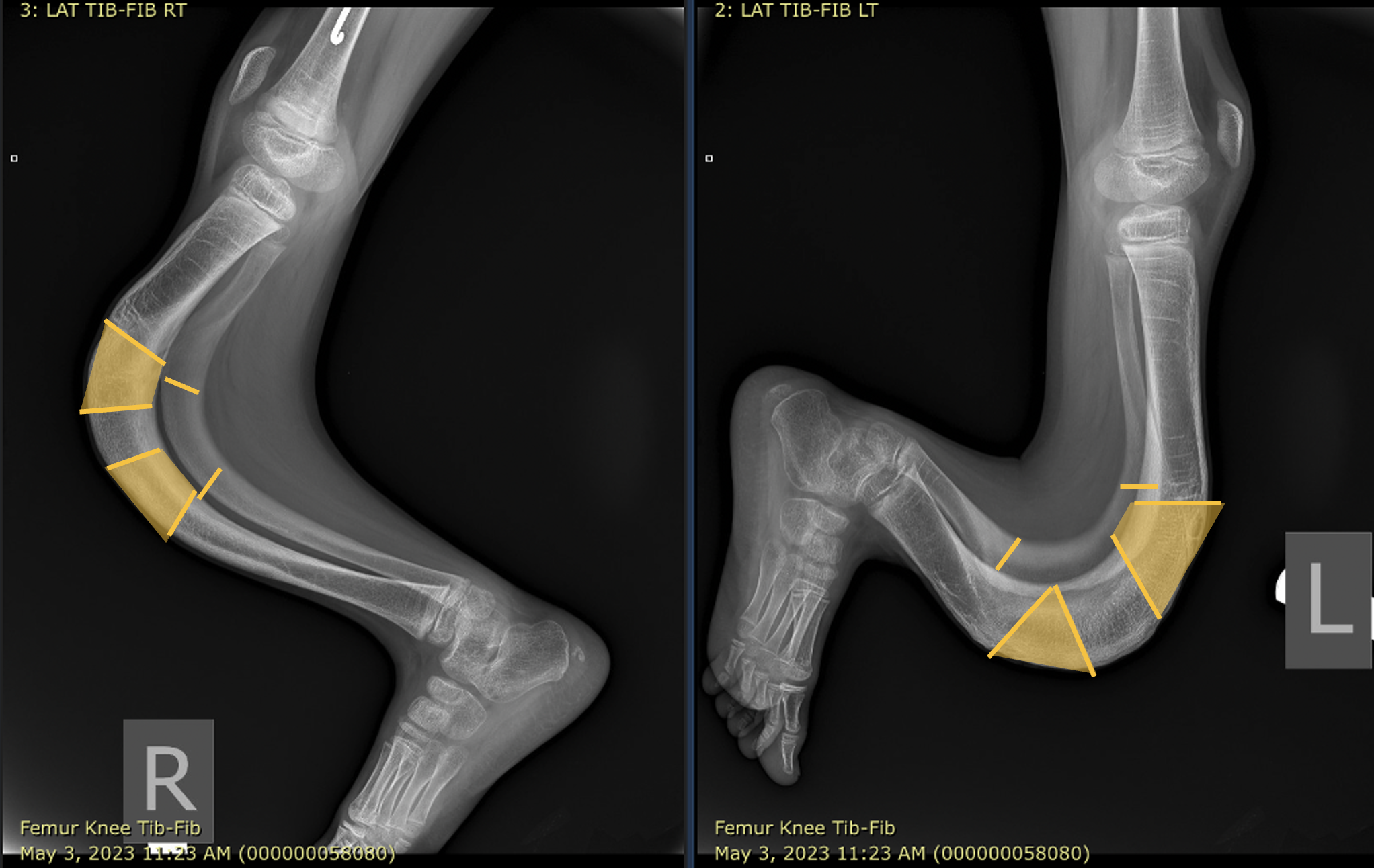
Pre-op x-ray shows the plan to remove shaded areas of the tibia, cutting each bone in four or more places to straighten. One or more intervening pieces are cut square to place in between the upper and lower part of the bone. This is called the shish kabob technique, as the pieces of bone are placed on the rod that holds them stable. Part of the fibula (small bone) is also removed. Then we used an external fixator to stabilize the rotation. Dealing with soft tissues, swelling, and wound healing can be challenging.

After a two-hour operation.

One month after surgery, walking with our physical therapist
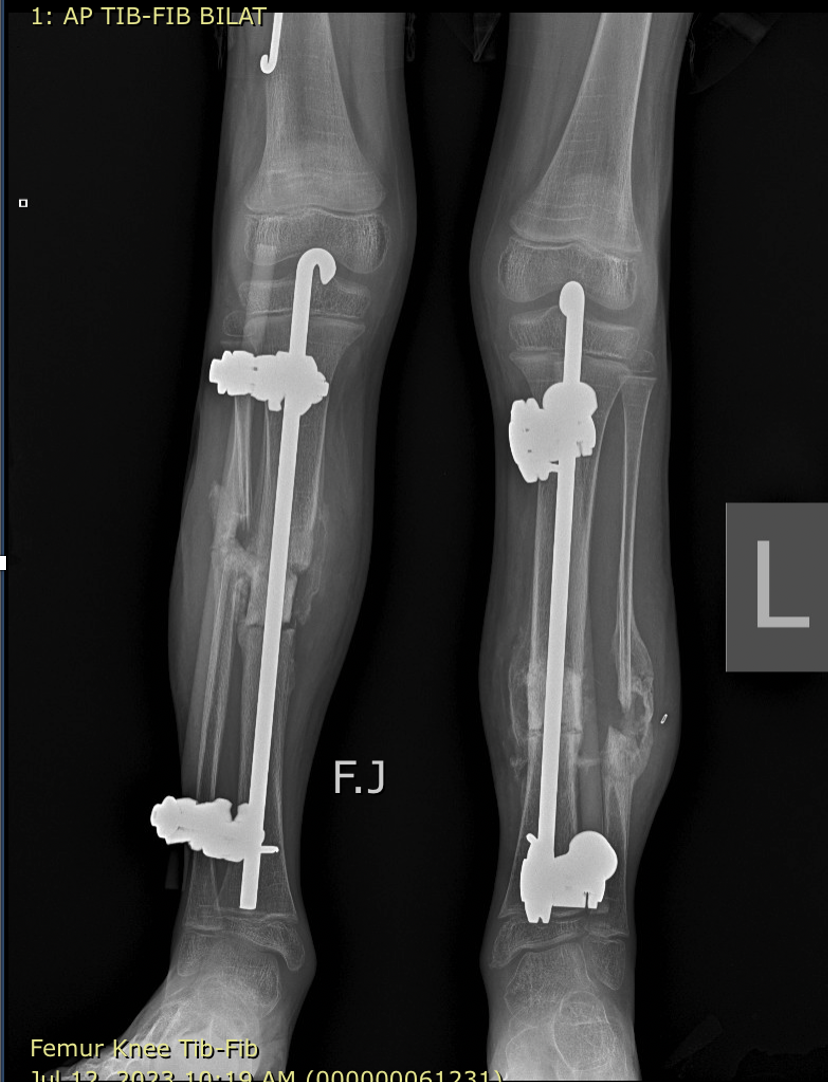
Two months after surgery, the shish kabob is healing well (front views), and walking is getting easier. The external fixators can be removed.
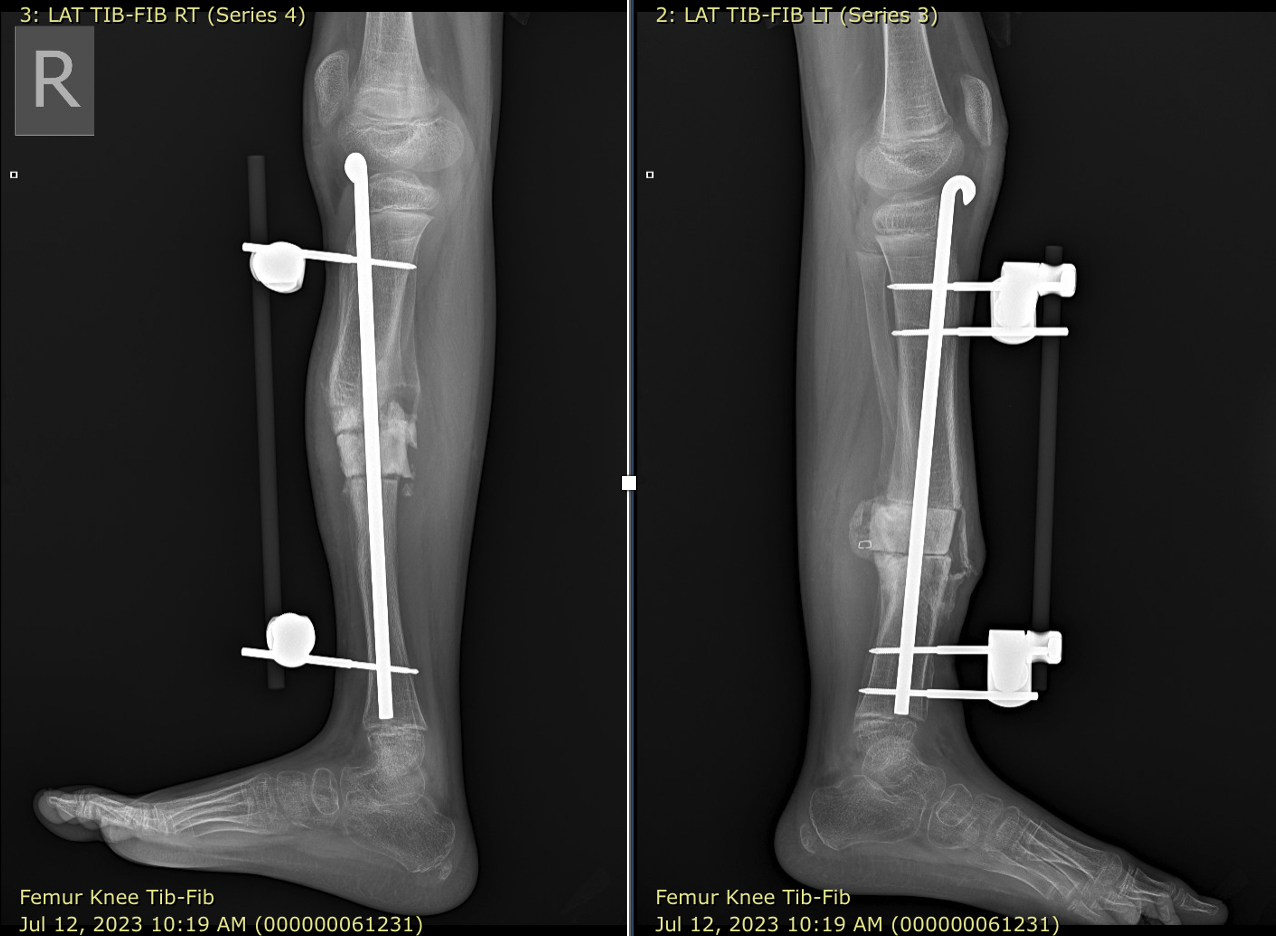
Side view, two months after surgery.





Recent Comments